A complete, honest guide to what your two-year-old is — and should be — doing right now
My son Eli turned two on a Tuesday. By Wednesday afternoon I was deep in a Google rabbit hole comparing his vocabulary count to developmental charts, half-convinced that the fact he still hadn’t mastered two-word sentences was a sign of something I had missed, something I should have caught earlier, something I should be doing differently.
By Thursday I had called our pediatrician’s office three times, read seven conflicting articles, and joined two parenting forums where mothers posted things like “my daughter has a 300-word vocabulary at 22 months” — which is wonderful for her daughter and absolutely demolished what remained of my peace of mind.
If you are reading this article, there is a reasonable chance you are sitting somewhere in that spiral right now. And I want to say this clearly before we go any further: the fact that you are paying attention, asking questions, and trying to understand your child’s development is one of the most protective things you can do for them. You are already doing it right.
What I’m going to give you here is what I wish I had found on that Wednesday — a clear, comprehensive, honest guide to what two-year-olds are typically doing developmentally, what the range of typical looks like, and the specific signs that genuinely warrant a conversation with your pediatrician. No panic. No comparison traps. Just useful, accurate information presented with warmth.
What “Typical” Actually Means at Age Two
Before we go through the milestones, I want to spend a moment on the word “typical” — because the way it’s used in developmental literature is often misunderstood by parents, and that misunderstanding is the source of enormous unnecessary anxiety.
Developmental milestones are not a checklist that every child completes on exactly the same schedule. They are ranges — derived from large-scale studies of child development — that describe what most children can do by a certain age. The word “milestone” refers to a skill that most children (roughly 75–90% of children, depending on the milestone) have acquired by a particular age.
This means that a significant minority of children — completely healthy, typically developing children — have not yet reached certain milestones by the age associated with them. A child who achieves a milestone somewhat later than average is not automatically cause for concern. What matters are patterns, trajectories, and combinations of signs — not a single isolated skill.
Two-year-olds vary enormously — and this is genuinely normal. One typical two-year-old may have a vocabulary of 50 words; another typical two-year-old may have 300. One may be combining words confidently; another may still be working on it. The range of “typical” at age two is genuinely wide, and falling anywhere within that range is not a cause for concern. What the red flags section of this article addresses are patterns that fall outside that range in ways that suggest a developmental evaluation would be helpful.
With that framing in place — let’s go through the milestones, domain by domain.

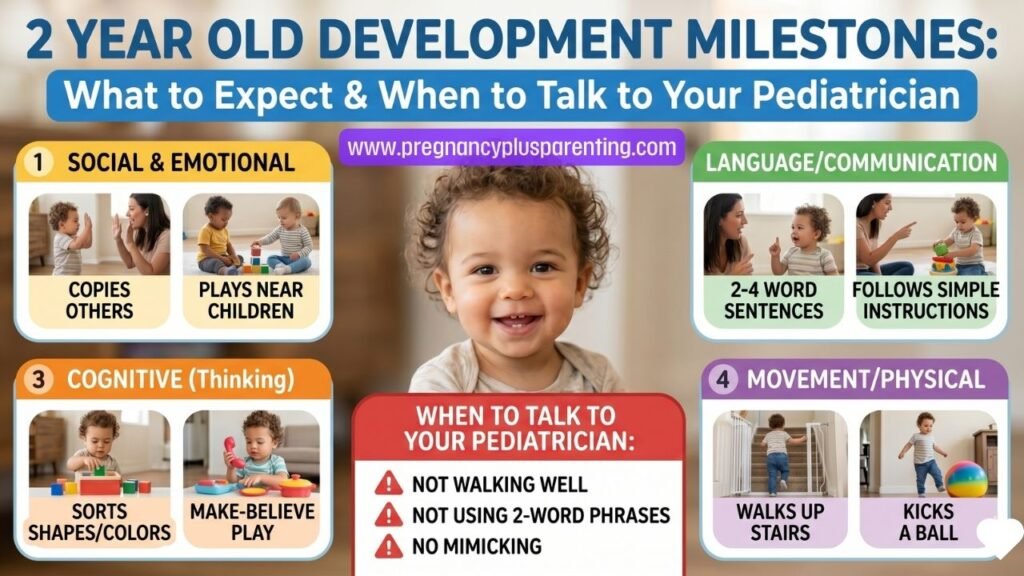
Language & Communication Milestones
Language development is often the domain parents are most aware of — and most anxious about — at age two. It is also the area where early intervention, if needed, makes the most significant difference. Here is what the research-based milestones look like for language between 24 and 30 months:
Most important domain
Typical
Typical
Typical
Typical
Typical
Typical
Emerging
Emerging
When counting your toddler’s words for the 50-word milestone, count any word or consistent word-like sound your child uses meaningfully and consistently — animal sounds that are used to label (saying “moo” to mean cow), names of family members, and even made-up words used consistently. The milestone is about intentional, consistent communication — not perfect pronunciation.
Gross and Fine Motor Milestones
Motor Development — Gross & Fine Motor at Age 2
Physical development
Typical
Typical
Typical
Typical
Typical
Typical
Typical
Emerging
Cognitive & Thinking Milestones
Cognitive Development — Thinking & Learning at Age 2
Brain development
Typical
Typical
Typical
Typical
Typical
Typical
Typical
Typical
Social & Play Milestones
Emotional Development Milestones
Emotional Development — Feelings at Age 2
Big feelings stage
Typical
Typical
Typical
Typical
Typical
What a Developmentally Rich Day Looks Like
You don’t need elaborate activities, expensive toys, or a Pinterest-perfect schedule to support your two-year-old’s development. Here is what a genuinely developmentally rich ordinary day looks like:
Red Flags — When to Talk to Your Pediatrician
The following signs, observed consistently and not explained by temporary illness or environmental disruption, are worth discussing with your pediatrician. This list is not meant to cause panic — it is meant to help you have an informed, specific conversation with your child’s doctor when you have concerns.
Fewer than 50 words at 24 months
A vocabulary of fewer than 50 words by the second birthday is a significant language milestone that warrants a speech-language evaluation. Early speech therapy is highly effective and outcomes are significantly better with early intervention.
Discuss now
No two-word combinations by 24 months
Combining two words — “more juice,” “daddy come” — is a critical language milestone. The absence of two-word phrases by 24 months is a well-established indicator that a speech evaluation is warranted.
Discuss now
Limited or inconsistent eye contact
Not maintaining eye contact during interaction, or doing so inconsistently, can be associated with a range of developmental differences including autism spectrum disorder. Combined with other signs, warrants evaluation.
Discuss now
Not responding consistently to their name
By 12 months a child should reliably respond to their name. If your 2-year-old frequently does not respond when called by name — not due to hearing, not due to being focused — this deserves pediatric attention.
Discuss now
Loss of previously acquired skills
Regression in skills your child had already developed — loss of words, loss of social engagement, loss of motor skills — is always worth immediate discussion with your pediatrician. This is different from temporary regression during stress.
Discuss now
No pretend play by 24 months
Pretend play is an important marker of symbolic thinking. A complete absence of any pretend play — feeding dolls, pretending to cook, using objects symbolically — warrants discussion, particularly alongside other social or language differences.
Discuss soon
Very limited interest in other people or other children
While 2-year-olds are not expected to play cooperatively, complete disinterest in other people — no seeking of connection, no social referencing, no interest in peers — is worth discussing with your doctor.
Discuss soon
Concerns about hearing
If you have any concern at all about your child’s hearing — they don’t seem to respond to sounds, don’t turn toward voices, or language development seems significantly delayed — request a hearing evaluation. Hearing loss is an easily missed but very treatable cause of language delay.
Discuss nowTantrums that are extremely frequent, long, or include self-injury
Frequent daily tantrums lasting 30+ minutes, tantrums that include head-banging or self-harm, or a child who cannot be calmed after a meltdown warrants discussion. This may indicate a sensory processing difference, anxiety, or other developmental consideration.
Discuss soon
Significant motor delays or coordination concerns
Not walking by 18 months, persistent toe-walking, significant coordination difficulties, or regression in previously acquired motor skills all warrant pediatric evaluation and possible referral to occupational or physical therapy.
Discuss soon
If something about your child’s development concerns you — even if you can’t articulate precisely what — trust that instinct enough to bring it to your pediatrician. You know your child better than anyone. A parent who says “something feels different” is frequently right. You are not being an anxious parent by asking. You are being an attentive one. Early evaluation and early intervention, when needed, make a real and lasting difference.
Typical vs. Concerning — A Side-by-Side Look
Here is a clear side-by-side comparison of typical two-year-old behavior versus signs that warrant professional evaluation:
Has intense tantrums but eventually calms with parental support
Plays alongside other children (parallel play) rather than with them
Shows separation anxiety but can eventually separate with support
Very picky about food, clothes, routines — strong preferences
Engages in pretend play — feeds doll, “drives” toy car, “cooks”
Makes eye contact naturally during interaction and play
Speech understood by familiar adults 50–75% of the time
Fewer than 50 words at 24 months or no two-word combinations
Tantrums lasting 30+ minutes consistently, or include self-harm
No interest in other children or other people at all
Extreme, persistent separation anxiety that does not reduce at all over time
Complete rigidity — extreme distress at any change, routine disruption
No pretend play of any kind at 24+ months
Inconsistent or absent eye contact during interaction
Speech mostly unintelligible even to familiar adults
What to Do If You Are Worried
If you have read through this article and have specific concerns about your child’s development, here is a clear, step-by-step approach:
Write down exactly what you are observing
Before you call your pediatrician, spend a few days noting specific observations: “She has approximately 30 words I can count.” “He has never combined two words together.” “She doesn’t respond when I call her name from another room.” Specific, concrete observations are far more useful to a clinician than “I’m worried about development.” They also help you organize your own thinking.
Request the 24-month developmental screening at your well-child visit
The 24-month well-child visit includes a standardized developmental screening — typically the M-CHAT-R/F for autism spectrum disorder and a broader developmental questionnaire. If you have concerns, make sure this screening happens and ask about the results explicitly. If your child is not yet due for their 24-month visit, call and ask for an early appointment to discuss developmental concerns — pediatricians take these calls seriously.
Ask for a referral to early intervention or a specialist
In the United States, children under 3 with developmental delays are eligible for free early intervention services under Part C of IDEA (Individuals with Disabilities Education Act). You do not need a diagnosis to receive an evaluation — a delay or concern is sufficient. Ask your pediatrician for a referral, or in most states you can self-refer by contacting your state’s early intervention program directly. Early intervention services typically include speech therapy, occupational therapy, and developmental support.
If your pediatrician dismisses your concern — advocate
“He’ll catch up” or “Let’s just wait and see” are responses that are sometimes appropriate — and sometimes not. If your pediatrician dismisses a concern that feels significant to you, you are absolutely entitled to seek a second opinion or to ask specifically: “What would need to be happening for you to refer us for a speech evaluation?” That question often changes the conversation.
Remember: early evaluation is not a verdict
Seeking an evaluation for your child’s development is not the same as receiving a diagnosis. An evaluation tells you where your child is — and if there is a gap, it opens the door to support that can make a genuine difference. Many children who receive early intervention go on to meet all milestones within a year or two. The earlier the support begins, the better the outcomes. There is no downside to asking.
How to Support Your Two-Year-Old’s Development at Home
You do not need special training, expensive programs, or elaborate equipment. Here are the evidence-based practices that most support development across all domains at age two:
Talk to your child constantly — narrate your day. “Now I’m putting the red cup in the dishwasher. The water is warm.” This running commentary is one of the highest-impact language development practices available, and it costs nothing. The more language-rich your child’s environment, the more language they develop.
Read together daily — and make it interactive. Point at pictures. Ask “what’s that?” Ask “what do you think will happen next?” Name characters’ emotions. Read the same books repeatedly — repetition builds vocabulary and comprehension. Aim for at least 15–20 minutes of shared book reading per day.
Provide open-ended play materials. Blocks, playdough, sand, water, simple art supplies, and basic pretend play items (toy food, dolls, vehicles) support cognitive, creative, fine motor, and social development far more effectively than batteries-required electronic toys. Let them lead the play. Resist the urge to direct or “teach” during play — follow their interest.
Give them time outdoors every day. Outdoor play supports gross motor development, sensory processing, creativity, and wellbeing. Children who spend time outdoors regularly show better physical development, better sleep, and — interestingly — better cognitive outcomes than those who don’t. Even 30 minutes of genuine outdoor time daily makes a difference.
Name emotions — constantly, in all situations. “You’re frustrated because the block fell.” “You feel so excited to see Grandma!” “Mama is feeling sad today.” Emotional vocabulary builds emotional regulation capacity. Children who have words for their feelings are better able to manage those feelings — this is not philosophy, it is well-documented neuroscience.
Limit screens — especially solo screen time. The American Academy of Pediatrics recommends limiting screen time for 2-year-olds to 1 hour per day of high-quality programming, watched together with a caregiver who talks about what’s happening on screen. Solo, passive screen consumption does not support language or cognitive development at this age.
Let them do things themselves — even slowly, even messily. Letting your toddler pour their own water, put on their own shoes, help carry groceries, stir the batter — these moments of competence and independence build both fine motor skills and self-confidence. The developmental benefit of letting them try is worth every spill.
The most developmentally powerful thing most parents can do for their two-year-old is not a program or a curriculum. It is presence: engaged, warm, language-rich, consistent presence.
— Early childhood development research consensus
FAQ from Worried Parents
The fact that your child understands language (receptive language) is a very positive sign — it tells you that language comprehension is developing. However, the gap between understanding and speaking can occasionally mask a genuine expressive language delay. If your child is under 50 words at 24 months or not combining words, the fact that they understand well doesn’t mean the gap should be ignored — it means the evaluation will likely have positive findings, and speech therapy, if recommended, has excellent outcomes for children with primarily expressive delays.
Temporary regression in language can happen during periods of stress, illness, major transitions, or developmental leaps — and is usually short-lived. However, a genuine loss of previously acquired language skills — words that were consistently in your child’s vocabulary and then disappeared — is always worth discussing with your pediatrician promptly, particularly if accompanied by changes in social engagement or behavior. This is one of the more significant red flags in toddler development and warrants timely evaluation.
Trust your instinct and advocate. You can request a specific referral — “I would like a referral for a speech-language evaluation” — rather than asking whether one is needed. You can also self-refer to your state’s early intervention program (in the US) without a doctor’s referral. And you can seek a second opinion from a developmental pediatrician. Your concerns as a parent who knows your child are valid data. The phrase that often helps: “I understand you’re not concerned, but I would feel much better with an evaluation. Can you please refer us?”
No. Potty training is not a developmental milestone in the same way that language, motor, and social milestones are — it is a skill that depends on both developmental readiness and intentional teaching, and readiness varies enormously between children. The typical range for potty training completion is anywhere from 22 months to 3.5 years. A child who is not potty trained at age two is completely within the normal range. The developmental readiness signs — showing awareness of being wet or soiled, some ability to wait, interest in the toilet — typically appear between 18 and 30 months.
Tantrums at age two are expected and normal — they are the expression of emotional experience that exceeds regulatory capacity. What distinguishes typical tantrums from those worth discussing with a pediatrician are: frequency (multiple very severe tantrums every day, consistently), duration (regularly lasting more than 30–45 minutes), content (tantrums that include deliberate self-harm such as head-banging on hard surfaces, or significant harm to others), and recoveryability (a child who cannot be calmed at all even after a long period). If tantrums are intense and frequent but the child recovers and is otherwise developing typically — that is exhausting, but it is within the range of normal.
Absolutely — uneven developmental profiles are extremely common and completely normal in typical development. A child might have an exceptionally advanced vocabulary but average motor development. A child might be a physical daredevil with developing language skills. Development is not a uniform progression across all domains simultaneously. What matters is that each domain is progressing over time, and that no domain shows the specific red flags described in this article. Unevenness across domains is standard human development, not a sign of a problem.
Every Child Has Their Own Timeline — A Final Word
Eli — my son who launched me into that Wednesday spiral — began combining words at 25 months. By 28 months he had not stopped talking, at remarkable length, about vehicles of all kinds. He is five now and recently explained to his kindergarten teacher, unprompted, exactly how a diesel engine works.
I share this not to offer you false reassurance — some children do need support, and seeking that support is not a failure, it is advocacy — but to remind you that development is not a race with fixed checkpoints that must all be reached at the same moment.
Your child is a unique person with their own developmental pace, their own strengths, their own emerging personality. The milestones in this article describe what most children do most of the time — they are not a verdict on any individual child’s worth or potential.
Pay attention. Trust your instincts. Ask questions without embarrassment. Seek evaluation if something concerns you — and seek it early, because early really does matter if support is needed.
And then, on the ordinary days, just be with your two-year-old. They are in the most extraordinary season of human development. It is exhausting and messy and sometimes genuinely hard — and it is also remarkable.
You are watching a person become themselves. That is something worth being present for.
Resources Worth Bookmarking
CDC Developmental Milestones (cdc.gov/milestones) — the CDC’s free, research-based milestone checklists updated in 2022, available as a free app (CDC Milestone Tracker) for tracking your child’s development over time.
ASHA (American Speech-Language-Hearing Association) (asha.org) — the professional association for speech-language pathologists, with parent-friendly resources on communication milestones and how to find an SLP in your area.
Early Intervention — contact your state or local early intervention program to request a free developmental evaluation if your child is under 3 and you have concerns. In the US, the Child Find system is federally mandated to evaluate and serve children with developmental delays regardless of income.
American Academy of Pediatrics (healthychildren.org) — the AAP’s parent-facing site with detailed, evidence-based information on child development by age.
This article is written to be informative and supportive — it is not a substitute for the individualized assessment of a pediatrician, developmental pediatrician, or other qualified clinician who knows your child. If you have concerns about your child’s development, please bring them to your child’s healthcare provider. This article can help you have that conversation more effectively — it cannot replace it.